
Abdominal Exam II: Percussion
Обзор
Source: Alexander Goldfarb, MD, Assistant Professor of Medicine, Beth Israel Deaconess Medical Center, MA
Medical percussion is based on the difference in pitch between the sounds elicited by tapping on the body wall. The auditory response to tapping depends on the ease with which the body wall vibrates, and is influenced by underlying organs, strength of the stroke, and the state of the body wall. There are three main medical percussion sounds: resonance (heard over lungs), tympany (heard over the air-filled bowel loops), and dullness (heard over fluid or solid organs). The contrast between dullness vs. tympany or resonance allows for determination of the size and margins of organs and masses, as well as identification of fluid accumulation and areas of consolidation. Percussion remains an intricate part of the physical diagnosis since it was first introduced more than 200 years ago, and is especially useful in examination of the lungs and abdomen.
As a part of an abdominal examination, percussion follows visual inspection and auscultation. The examiner should first percuss over each of the nine abdominal regions (epigastric region, right hypochondriac region, left hypochondriac region, umbilical region, right lumbar region, left lumbar region, hypogastric region, right inguinal region, and left inguinal region). Tenderness elicited by percussion is abnormal, and peritoneal inflammation should be suspected. As the air-filled bowel loops are positioned in the closest proximity to the abdominal wall, the percussion over most parts of the abdominal cavity elicits a predominantly tympanic sound. The presence of large areas of dullness should prompt evaluation for organomegaly, intra-abdominal masses, or fluid.
In addition to assessing the amount and distribution of abdominal gas, an abdominal exam should include an estimation of liver and spleen size by percussion. As the liver and spleen are covered by the rib cage, the examiner should percuss over the lower anterior chest as well. Normally, one expects to hear dull sound on percussion of the right anterior chest over the liver, and tympanic sound on percussion of left anterior chest over the gastric air bubble and the splenic flexure of the colon (Figure 1).
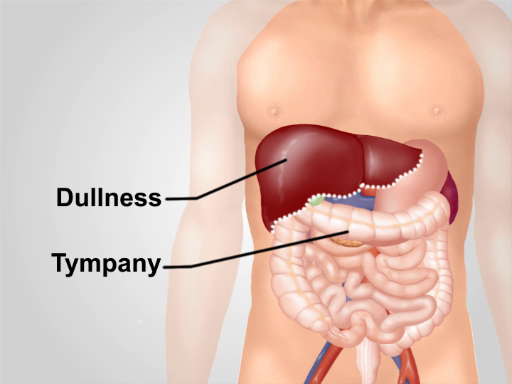
Figure 1. Normal percussion notes over abdominal region. With the exception of an area of dullness over the liver in the right lower anterior chest, tympany is the predominant sound heard over the region.
Процедура
1. General percussion of the abdomen
- Explain the procedure to the patient
- Perform light percussion over each of the nine abdominal regions.
- As you percuss, watch the patient's face for any signs of discomfort. Ask the patient if they are experiencing any tenderness. Tenderness on percussion is abnormal and can indicate peritoneal inflammation.
- Listen to the intensity, pitch, and duration of the percussion note. Normally, tympanic sound produced by air in the bowel loops will be heard. Tympanic sound is relatively long, high pitched, and loud. Occasional areas of dullness (lower pitched, shorter, and quieter sound than tympany) are produced by fluid and feces, and are normal as well. Large areas of dullness suggest an enlarged organ or a mass that has to be further assessed by palpation and additional maneuvers.
- Percuss the lower anterior chest above the costal margins. Normally the spleen and liver are covered by the rib cage, with the liver edge occasionally found 1-2 cm below the costal margin. Dull sound on the right over the liver is expected. On the left, tympany over the gastric air bubble and the splenic flexure of the colon should be heard.
- Percuss above the pubic symphysis. Dullness on percussion in this area indicates an enlarged uterus or distended bladder.
2. Determine the liver span
Increased liver span on percussion indicates an enlarged liver, which can underlie a variety of pathological processes. It is essential to identify both the lower and the upper borders of the liver dullness to distinguish between an enlarged liver (which has an increased span), and a liver displaced downwards as a result of chronic obstructive pulmonary disease (in which case the liver span is normal).
- Start by locating the right midclavicular line. Lightly percuss in the right midclavicular line upwards starting in the area of tympany below the umbilicus. Bending down to listen carefully to the percussion note might be required.
- Make a mark where the tympany changes to dullness (lower border) with a skin pencil.
- Percuss in the right midclavicular line downwards starting at the nipple line to identify an upper border of liver dullness.
- Mark the point on the abdominal wall where the resonant sound over the lungs changes to dullness over the liver with a skin pencil.
- Measure the distance between upper and lower border of dullness in cm. Liver span depends on age, sex, and body type. The liver span is normally 6-12 cm (mean liver span is 7 cm for women and 10.5 cm for men).
- If the liver span is increased, percuss laterally and medially. Normal liver span in the midsternal line is 4-8 cm.
3. Percuss left anterior chest to detect splenomegaly
The spleen is located slightly posterior to the left midaxillary line and produces an oval area of dullness between the 9th and 11th ribs. Only a small surface of a normal spleen is superficial enough to be detected, and the splenic dullness is often obscured by gastric or colonic tympany. However, an enlarged spleen is expanded towards the midline, anteriorly, and downward, and might be detected by two special percussion maneuvers: Traube's space percussion and/or Castell's maneuver.
- Percussion of Traube's space, anterior axillary line, and left costal margin.
- Along with the other pathological conditions medial expansion of an enlarged spleen can produce dullness on percussion over Traube's space.
- With the patient supine and their left arm slightly abducted, percuss from the medial to lateral border of Traube's space. Dullness on percussion or reduction of the area of tympany can result from splenomegaly.
- Castell's method (checking for a splenic percussion sign).
- Percuss in the anterior axillary line in the lower intercostal space.
- Ask the patient to take a deep breath, and percuss again. A normal-sized spleen is positioned above the percussion point even when it descends during inspiration, and the percussion tone is tympanic on both expiration and inspiration. If a percussion note is dull or becomes dull on inspiration (positive splenic percussion sign), splenomegaly is suspected (Figure 3).
4. Evaluation of protuberant abdomen.
Percussion is helpful to diagnose the causes of a protuberant abdomen. Tympany over a protuberant abdomen indicates air accumulation that could be due to an intestinal obstruction. When percussion over the flanks of a protuberant abdomen produces a dull note, it is consistent with fluid accumulation or ascites.
- Shifting dullness" maneuver is performed when ascites is suspected.
- With the patient in the supine position, percuss in a lateral direction from the umbilicus and make a mark of the point where the tympanic sound changes to dullness with the skin pencil.
- Ask the patient to roll onto the side (lateral decubitus position), and repeat the percussion, starting from the top, and make a second mark on the skin when the tympanic sound changes to dull. If abdominal fluid is present, the border of gas/fluid interface will be shifted upwards toward the umbilicus (Figure 2).
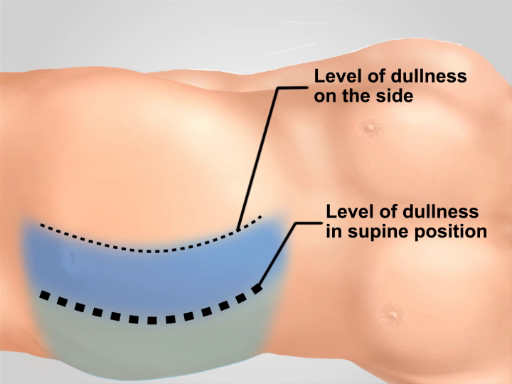
Figure 2. Shifting dullness test. If ascites is present, the point at which tympany changes to dullness over the abdominal flanks is shifted upward towards the umbilicus when the patient is in lateral decubitus position.
Заявка и Краткое содержание
Despite rapid advances in imaging techniques, abdominal percussion remains an essential part of a physical examination. Correct percussion technique is critical for this method to be effective. The percussion strike should be kept the same over the entire abdomen. All the information obtained during the patient's interview and full physical examination, and a good knowledge of differential diagnoses of each pathological sign is essential for proper interpretation of any findings. For example, a false increase of liver span on percussion can result from right lung consolidation and/or a pleural effusion. One should also be aware of the limitation of the method and the sensitivity of each diagnostic maneuver. While percussion is only moderately accurate in detecting hepato-and splenomegaly, abnormal findings should prompt further clinical evaluation.
Теги
Перейти к...
Видео из этой коллекции:

Now Playing
Abdominal Exam II: Percussion
Physical Examinations II
247.1K Просмотры

Eye Exam
Physical Examinations II
76.5K Просмотры

Ophthalmoscopic Examination
Physical Examinations II
67.2K Просмотры

Ear Exam
Physical Examinations II
54.4K Просмотры

Nose, Sinuses, Oral Cavity and Pharynx Exam
Physical Examinations II
65.2K Просмотры

Thyroid Exam
Physical Examinations II
104.2K Просмотры

Lymph Node Exam
Physical Examinations II
384.6K Просмотры

Abdominal Exam I: Inspection and Auscultation
Physical Examinations II
201.8K Просмотры

Abdominal Exam III: Palpation
Physical Examinations II
138.1K Просмотры

Abdominal Exam IV: Acute Abdominal Pain Assessment
Physical Examinations II
66.9K Просмотры

Male Rectal Exam
Physical Examinations II
113.6K Просмотры

Comprehensive Breast Exam
Physical Examinations II
86.6K Просмотры

Pelvic Exam I: Assessment of the External Genitalia
Physical Examinations II
303.6K Просмотры

Pelvic Exam II: Speculum Exam
Physical Examinations II
149.3K Просмотры

Pelvic Exam III: Bimanual and Rectovaginal Exam
Physical Examinations II
146.7K Просмотры
Авторские права © 2025 MyJoVE Corporation. Все права защищены