
Method Article
Therapy Testing in a Spheroid-based 3D Cell Culture Model for Head and Neck Squamous Cell Carcinoma
* Wspomniani autorzy wnieśli do projektu równy wkład.
W tym Artykule
Podsumowanie
We describe the evolution of a spheroid-based, three-dimensional in vitro model that enables us to test the current standard of experimental therapy regimens for head and neck squamous cell carcinoma on cell lines, aiming at evaluating therapy susceptibility and resistance on primary cells from human specimens in the future.
Streszczenie
Current treatment options for advanced and recurrent head and neck squamous cell carcinoma (HNSCC) enclose radiation and chemo-radiation approaches with or without surgery. While platinum-based chemotherapy regimens currently represent the gold standard in terms of efficacy and are given in the vast majority of cases, new chemotherapy regimens, namely immunotherapy are emerging. However, the response rates and therapy resistance mechanisms for either chemo regimen are hard to predict and remain insufficiently understood. Broad variations of chemo and radiation resistance mechanisms are known to date. This study describes the development of a standardized, high-throughput in vitro assay to assess HNSCC cell line's response to various therapy regimens, and hopefully on primary cells from individual patients as a future tool for personalized tumor therapy. The assay is designed to being integrated into the quality-controlled standard algorithm for HNSCC patients at our tertiary care center; however, this will be subject of future studies. Technical feasibility looks promising for primary cells from tumor biopsies from actual patients. Specimens are then transferred into the laboratory. Biopsies are mechanically separated followed by enzymatic digestion. Cells are then cultured in ultra-low adhesion cell culture vials that promote the reproducible, standardized and spontaneous formation of three-dimensional, spheroid-shaped cell conglomerates. Spheroids are then ready to be exposed to chemo-radiation protocols and immunotherapy protocols as needed. The final cell viability and spheroid size are indicators of therapy susceptibility and therefore could be drawn into consideration in future to assess the patients' likely therapy response. This model could be a valuable, cost-efficient tool towards personalized therapy for head and neck cancer.
Wprowadzenie
Head and Neck squamous cell carcinoma (HNSCC) is the sixth most common cancer worldwide with a rising incidence of mucosal human papillomavirus (HPV) infection-associated pathogenesis, next to a majority of cases caused by excessive nicotine and alcohol consumption 1,2. While smaller tumors and pre-invasive stages are usually well treatable with surgical excision, usually combined with cervical lymph node dissection, treatment for advanced-stage and recurrent HNSCC remains challenging due to aggressive tumor invasion with metastatic spread and resistance to radiation and chemotherapy protocols3,4,5,6,7,8. Recent studies suggest a high variability of cellular phenotype, and sub-characterization of circulating and disseminated tumor cells has just begun9,10. The earlier belief of a solid, uniform tumor mass had to be revised in the light of recent studies in the past years11,12,13,14. Current approaches for tumor characterization and identification of key mutations could identify several genes that seem to be associated with therapy resistance but remain a cost-intensive approach. Moreover, knowledge of genotype does not necessarily allow a reliable prediction of phenotype and its treatment response.
There have been few advances in improving overall and disease-free survival for advanced-stage and recurrent disease. For nicotine- as well as virus-associated carcinoma, current treatment options besides surgery enclose aggressive radiation and platinum-based chemotherapy regimens. There have been implications for different response rates between HPV-negative and positive carcinoma; however, this has not yet lead to a change in general therapy guidelines. Resistance towards radiation and chemotherapy is a widespread phenomenon in all tumor stages and exists for platinum-based chemotherapy as well as for targeted therapy (Anti-EGFR; epidermal growth factor-receptor) and recently emerging checkpoint inhibition15. Ineffective radiation and chemotherapy come at a high cost of significant patient morbidity in terms of dysphagia, mucositis, dry mouth and risk of decrease of renal or cardiac function among others. Predicting therapy response prior the decision of a general therapy concept for each individual patient seems to be the crucial goal, preventing unnecessary treatment concepts, side effects and costs.
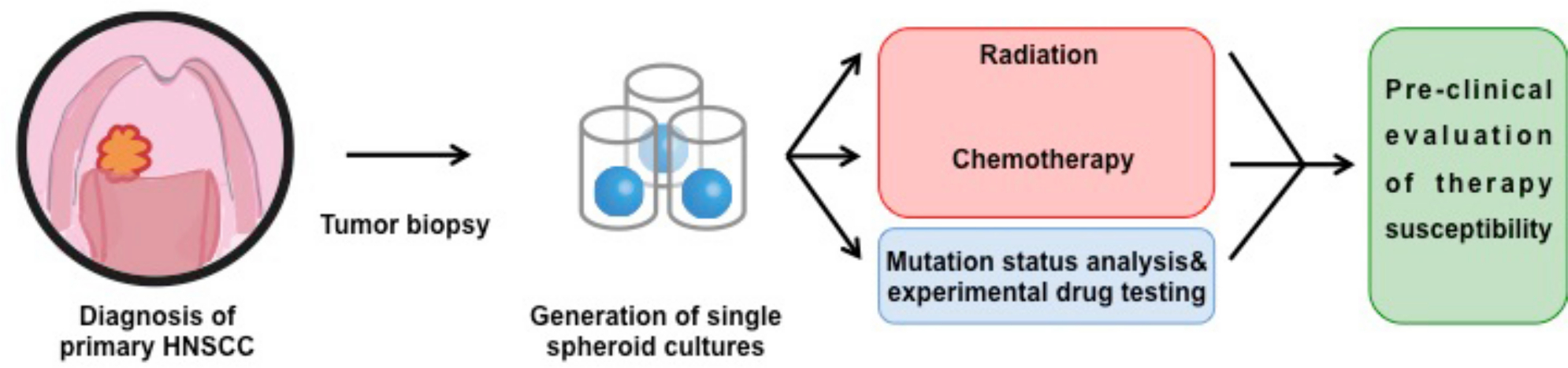
We sought to establish a model to test individual patient's treatment susceptibility towards current standard chemo-radiation that could be integrated into the regular and quality-controlled oncologic treatment algorithm from a technical standing point. The far goal was to use the model without using heavily altered and aged cell lines, as they poorly represent actual human tumor cells without their variability and heterogeneity as we know now, while establishment of the protocol was done in various cell lines. To be independent only from commercially available cell lines, we recently successfully generated an intermediate cell line called "PiCa" from primary HNSCC cells from human tumor specimens with conserved cellular markers on its surface and limited passages16. This PiCa cell line should serve as a preparation for the development of the model on the road to then later following trials with fresh human cancer cells from tumor biopsies. It has been shown that cells in three-dimensional cell cultures react differently and more in vivo-like to administration of cancer drugs than those growing in monolayers17,18,19,20,21, mainly due to conservation of migratory and sub-differentiation properties of certain cell subsets22,23,24. Here, we describe the protocol of a spheroid-based, three-dimensional model from intermediate cell lines and primary human squamous cell carcinoma cells and ways how integrate such a model into cancer treatment of the head and neck surgeon and oncologist (Figure 1).
Protokół
All studies shown in this manuscript, namely the use of human tumor specimens, are protected under and in consent with prior decisions from University Medicine of Mainz/University of Munich Medical Center Ethics committee. Patients have given informed consent according to national legal guidelines agreeing to scientific use of excess biological material that was obtained in the course of their treatment. Research has been performed in compliance with all institutional, national and international guidelines for human welfare.
1. Taking a Tumor Biopsy from Head and Heck Squamous Cell Carcinoma
- Perform general (propofol and/or sevoflurane, muscle relaxing agent) or local infiltration (2% ultracaine, adrenalin)/surface (xylocaine) anesthesia in the operating room or otolaryngology examination chair. Visualize the tumor mass in oral cavity/pharynx/larynx/other parts of the upper digestive and respiratory tract with standard operating instruments and, if needed, under the microscope.
- Take a fresh tumor biopsy from the periphery of the cancerous lesion with blunt or cutting instruments. Avoid the center of the lesion due to abundant necrosis in this area. Put the obtained tissue to a sterile container with isotonic sodium chloride solution.
- After the biopsy, perform hemostasis as needed, e.g., with a bipolar or monopolar coagulation device in addition to the use of vasoconstrictive substances.
- Bring the tumor biopsy intended to be used for cell culture experiments directly to the adjacent laboratory tract. Send other tumor biopsies to the pathologist as usual to rule out cancer.
- Make sure that a laboratory technician is ready to process the specimen directly.
2. Processing the Tumor Specimen
- Place the tumor specimen on a suitable and sterile surface and cut it thoroughly with a sterile single-use scalpel into as little as possible pieces.
Caution: Make sure the status of infectious and blood-borne diseases is well documented and the technician is in attention of the institutions standard protocols to prevent needle stick or cutting injury with potentially biohazard patient material and the protocols to follow after possible injury. - After sufficient mechanical separation of the primary tissue, put the tissue into a vial containing Collagenase I/II and incubate for 1 h at 37 °C. Sieve through a 70 µm falcon cell strainer and wash the suspension with Hanks' Balanced Salt solution (HBSS).
- After successful separation and subsequent washing, place the suspension containing 1-2 × 106 cells into a T75 cell culture flasks (75 cm2) to grow to sub-confluency at 5% CO2 and temperature of 37 °C. This step may take up to 10 days.
- Use special keratinocyte culture medium consisting of the following: 125 mL of Dulbecco's modified eagles medium (DMEM), 250 mL of Keratinocyte complemented medium (complemented medium consisting of 500 mL of Keratinocyte SF Medium, 15 mg of bovine pituitary extract (BPE), 2.5 mL of penicillin/streptomycin, 150 ng recombinant human epithelial growth factor (EGF), 516 µL of 300 mM CaCl2, stock mix to be prepared in advance), 125 mL of F12 nutrient mix, 10 mg of BPE (0.75 mL), 75 ng recombinant human EGF (2 µL), 3.75 mL of 200 mM L-Alanyl-L-Glutamin-Dipeptide (Table of materials).
3. Seeding the Cells into Ultra-low Adhesion Cell Culture Plates
- Confirm tumor cell growth under a microscope. Count the cells in culture (primary or cell culture) and seed 5,000 primary tumor cells or 1,000-2,000 cells of intermediate cell line/other cell line in 200-300 µL of media (step 3.2.) into an ultra-low adhesion plate with concave, round bottoms (96-well).
- Culture the cells at 5% CO2 at 37 °C and in equal parts DMEM and airway epithelial cell medium (BEGM), 10% fetal bovine serum, 1% penicillin/streptomycin, 1% sodium pyruvate, 1% non-essential amino acids, 1% L-glutamine (step 2.3.). If cell lines are being used, media on the basis of DMEM is sufficient.
- Perform media changes every other day. Pay attention not to aspirate the spheroid with the pipette during media changes. Culture the spheroids until the level of growth as descibed in 3.3 is reached (approximately 7-10 days).
- Confirm spontaneous spheroid formation under the microscope by looking for three-dimensional, spheroid-shaped cell conglomerates. Exclude the wells with irregular and/or multiple spheroid formation from further investigation.
NOTE: Spheroids should be visible with the naked eye, too, facilitating further processing and media changes as described below.
4. Exposing Spheroids to Multimodal Standard or Experimental Tumor Therapy
- Choose a desired therapy regimen. Design sufficiently large control groups that allow comparisons of treatments to untreated spheroids or spheroids receiving only partial therapy regimens, e.g. radiation alone. The size of control groups depends on the experimental group design and cannot be defined universally.
- Exchange the media to media with additives, meaning media with chemotherapeutics and/or monoclonal antibodies at desired concentrations. Add Cisplatin at the concentrations of 2.5/5/10 µM or 5-fluoruracil (5FU) at 30 µM.
NOTE: For high throughput experiments or large group sizes/large number of groups, one can use an automated pipetting robot as we are further establishing in the experiments. - Alternatively, radiate the cell culture plates with spheroids at 2 Gy using a suitable radiation facility.
Caution: Respect the institution's protocols regarding prevention of harmful radiation exposure of employees. Work only with designated and trained technicians according to radiation protection guidelines. If desired, add chemotherapeutics as described under 4.2. afterwards. - Incubate the cells for 24 h in previously described culture conditions (37 °C, step 3.2).
- After the incubation, continue the cell culture for at least 6 days with media changes every other day.
5. Assessment of Spheroid Size and Extent of Cellular Proliferation for Assay Read-out
- Measure the spheroid size in terms of area after digital photo documentation on day 6 (day 10, day 16) with a graphic software (parameter 1).
- After centrifugation at 520 x g for 2.5 min of the plate, remove the supernatant. Wash the cells with sufficient amount of 1x PBS and centrifuge the plate again as described, followed by removing the supernatant (PBS).
- Add 100 µL of enzymatic cell detachment solution to each vial to allow the spheroids to dissolve. Incubate the plate for 8 min at 37 °C.
- Check for successful dissolving of the spheroid under the microscope. Add 100 µL of DMEM. Centrifuge the plate at 520 x g for 2.5 min. Remove the supernatant and suspend the cells in 100 µL of DMEM.
- Perform a commercially available colorimetric proliferation assay, in example WST-8 assay on each vial according to the manufacturer's instructions25. Read out the assay in an enzyme-linked immunosorbent assay (ELISA) reader (parameter 2).
Wyniki
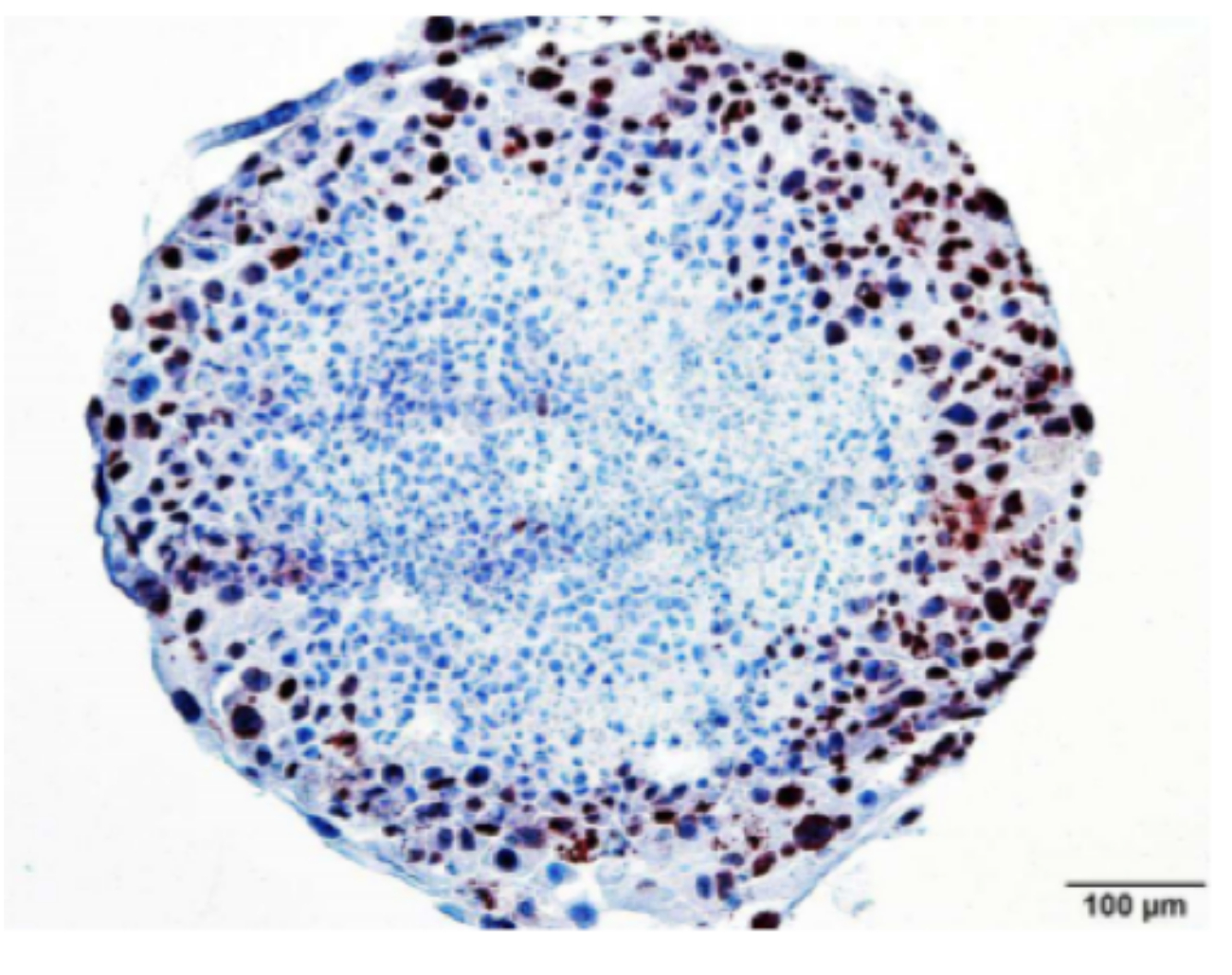
We were able to reproducibly generate spheroids from single cell suspensions, first from different cell lines including the proprietary PiCa cell line, later from primary human cancer cells derived from fresh tumor biopsies as described in Hagemann et al.26. We evaluated two established methods for spheroid generation; the two being the so-called hanging drop (HD) method and the ultra-low adhesion (ULA) method, the latter being the more effective and safe one. We were able to highlight the advantages of the ULA method compared to HD, including faster spheroid growth, fewer issues with plate handling, consequent loss of spheroids with heavy vibrations, and more reproducible spheroid growth in terms of uniformity (Figure 2). The occurrence of multiple spheroids per vial was more common in the HD method. We checked for a more distinct characterization of spheroid morphology. Figure 3 shows an immunochemistry staining for Ki67, a proliferation marker, of a spheroid from PiCa cells. As described in literature, spheroids consist of a less proliferating core with a proliferating outer layer, mimicking different regions of proliferation of solid HNSCC in humans. In vitro as in vivo, this is supposedly caused by a gradient of nutrients and oxygen supplied by the cell culture media causing a decrease from the periphery to the center of the tumor.
We then tried to show that the assay is able to detect variations in spheroid size after the incubation with chemotherapeutic drugs or exposure to ionizing radiation, here representing two common standard treatment regimens for HNSCC. Before possibly integrating the assay into a pre-treatment routine, the validation of the sensitivity of the assay would be a prerequisite. Two parameters were available as end points of the assay: spheroid size (area; parameter 1 from step 5.1.) and proliferation (see parameter 2 from step 5.4.), being a surrogate marker for cell viability and growth potential after therapy. The results of the treatment studies with common chemotherapeutic and chemo-radiation protocols are shown in Figure 4. Exposure and incubation of the spheroids with cisplatin or 5FU led to a significant reduction in growth speed over time compared to an untreated control group (p<0.001). Radiation with 2Gy was able to reduce growth speed in a significant manner (p<0.01). The survival assay (WST-8) was able to detect an additional, significant value of chemo-radiation with cisplatin compared to radiation alone (p = 0.017), a previously undetected difference in the assessment of spheroid size. This underlines its importance for the assay as a whole, augmenting its sensitivity for small changes therapy response.

Figure 1: Concept of a model on the way to future personalized therapy. Patients with either background of mucosal HPV infection and/or history of tobacco and alcohol abuse present to our tertiary referral care center for suspected diagnosis of head and neck cancer. Biopsies of suspicious mucosal areas or macroscopic tumor masses are taken under anesthesia to secure diagnosis. Additionally, we take tumor biopsies to generate three-dimensional spheroid-shaped cell cultures in the laboratory. Upon sufficient growth of primary-cell based spheroids, we expose them to current standard or experimental treatment regimens to test for individual therapy response. Further analyses of genetic or molecular variations can be added after analysis of therapy results. Therapy results in vitro can be drawn into consideration for the process of planning therapy concepts for the patient. This figure is reprinted from Hagemann, J. et al.26, with permission granted by authors and journal. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: All cell lines could generate reliable spheroids; differences in size and time of read-out are according to Figure 1. In preliminary experiments, primary cells did not form reproducible spheroids in HD but ULA plates (bottom left). Further studies are to be undertaken to evaluate spheroid growth characteristics from primary cells. The number of cells on the right is the initial number of cells put in the vial to form a spheroid. This figure is reprinted from Hagemann, J. et al.26, with permission granted by authors and journal. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Ki67 immunochemistry staining of a spheroid slice (PiCa). The periphery of the culture shows much higher proliferation rates than central cells, mimicking nutrient distribution in solid mucosal tumors that often show necrotic cores. This figure is reprinted from Hagemann, J. et al.26, with permission granted by authors and journal. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Therapy studies. (A) PiCa cells were cultivated to generate spheroids (n = 12 per group) in ULA plates. Cells were stimulated according to the protocol with either PBS as control, cisplatin at 5 µM or 5FU at 30 µM. Sizes of the spheroids were determined at day 6, 10 and 16 according to standard protocols. Cisplatin and 5FU treatment led to a significant decrease in size (p-values are given at left bottom in section (B) Identical experimental design as in (A) (n = 12), but with additional radiation of 2Gy. (C) Plot shows min to max. According to the p-values given in (C), previous radiation with 2Gy led to a significant decrease in spheroid size in the control group, imitating radiation therapy and showing radiation sensitivity of PiCa cells. Radiation in combination with cisplatin treatment did not lead to a further significant decrease in size of the spheroid (p>0.05). Plot shows min to max. (C) Calculated p-values from 2-way ANOVA analysis from experiments A and B. (D) WST8 assay performed on day 16 as an alternative for planimetric (area) analysis of the spheroids. WST8 analyses were able to detect a significant decrease in living cells after chemo-radiation (2Gy radiation and cisplatin) compared to cisplatin alone (p = 0.017), hence showing the advantage of combining both planimetric analysis and WST8 colorimetric assay at the time of assay read-out. Plot shows min to max. This figure is reprinted from Hagemann, J. et al.26, with permission granted by authors and journal. Please click here to view a larger version of this figure.
{kind=link}
Dyskusje
We were able to establish a protocol to generate reproducible spheroids from cell suspensions, for both cell lines and, in preliminary experiments, primary human tumor cells. We first assessed two previously described methods and identified the ULA-method, a method where culture plates with ultra-low adhesion surfaces are used, to be the safer and more reliable one for the generation of uniform three-dimensional spheroids. By combining two separate methods for assay read-out (size/area and cell viability), this multimodal assay is sufficiently sensitive to identify small differences between groups. This is the first step towards the proof of technical feasibility for later integration of the assay into the clinical pathway at our tertiary care center. In future, it could be used to (i) assess individual tumor susceptibility to common first- or second-/third-line therapy protocols (chemo-reagents, radiation) and experimental therapy protocols, (ii) further characterize the tumor cells from fresh specimens and correlate molecular surface or cytoplasmic patterns to therapy response. Spheroids from specimens coming from different tumor localizations, e.g., primary and lymph node metastasis, are imaginable.
Throughout the establishment of the protocol and method, we used different known cell lines, a few being well established for decades. The mere age of the cell lines raises the doubt of their connection and comparability to current actual human tumor cells, supposedly having lost several properties and hallmark molecular markers. Results from in vitro experiments were difficult to reproduce in human or in vivo trials27. We therefore focused on a cell line recently generated from human primary tumor cells in our facility that is well characterized16. With this cell line PiCa, we were able to conduct treatment experiments at a larger scale and confirmed current therapy expectations. This supports the theory that PiCa cells reflect actual human tumor behavior better than other, more aged and passaged cell lines that underwent numerous passages. Cells that may undergo non-physiological selection due to long-term in vitro conditions might bias chemo-radiation sensitivity. In recent experiments, we confirmed the feasibility with primary cells in regards to reliable spheroid formation; however, further and larger experiments have to be performed before being able to implement the assay into clinical routine.
It is assumed that spheroids and three-dimensional cell culture in general react differently compared to conventional 2D-culture when exposed to chemotherapeutic drugs or radiation 28. The architecture of spheroids leads to a gradient of oxygen and nutrition delivery from outer surface to core, and recent studies have shown that also drug delivery to different parts of the three-dimensional cell cluster is not uniform29. Furthermore, cells in spheroid culture seem to preserve certain gene expression patterns that are associated with drug resistance in animal models 30. We suggest that also so-called radiation resistance, a feature that has been linked to head and neck cancer in numerous patients, is a result of cell-cell interaction and distinct microenvironments leading to variations in oxygen supply and metabolic activity. This phenomenon could be mimicked in spheroids due to an increased in vivo functionality. In conclusion, the use of primary cells and the generation of spheroids could allow us to preserve as many as possible characteristics of in vivo tumor growth in combination with a cost-efficient assay for studying individual therapy response.
There certainly are limitations to the approach. To date, it is unknown how cells from different individual patients will perform in the assay being exposed to tumor treatment, and how predictive the assay is in terms of correlation with later therapy outcome. Excessive studies are necessary to simply compare the performance in vitro vs. clinical course. Among others, namely two factors contribute to this uncertainty: tumor heterogeneity and lack of co-culture with stromal and immune cells. Tumor heterogeneity is a not entirely understood phenomenon and exists between different sub-sites of the primary, as well as between primary and metastatic localization12. Since recent studies, there is a third site where very distinct and specialized tumor cells can exist and prevail in niches: blood and bone marrow are able to house circulating and disseminated tumor cells9,10. The lack of other cell types like stromal cells and T-cells (as a representative for the immune system) in cell culture is not limited to the assay, but a valid disadvantage of most in vitro assays studying tumor therapy susceptibility. In the light of recent drug approvals and ongoing studies that influence T-cell response, future experiments for drug discovery must be conducted in a combination of different assays and methods.
Ujawnienia
The authors have nothing to disclose.
Podziękowania
This project was funded by a grant of the University of Munich (FöFoLe project-no.: 789-781).
Materiały
| Name | Company | Catalog Number | Comments |
| Dulbeccos modified Eagles medium (DMEM) | Biochrom, Berlin, Germany | F 0425 | |
| Fetal bovine serum | Gibco Life Technologies, Paisley, UK | 10500-064 | |
| penicillin/streptomycin | Biochrom, Berlin, Germany | A2212 | |
| sodium pyruvate | Biochrom, Berlin, Germany | L0473 | |
| non-essential amino acids | Biochrom, Berlin, Germany | K0293 | |
| L-Glutamine | Biochrom, Berlin, Germany | K0293 | |
| Liberase | Roche Life Sciences, Basel, Switzerland | 5401127001 | |
| GravityPLUS 3D Culture and Assay Platform | InSphero, Schlieren, Switzerland | PB-CS 06-001 | |
| GravityTRAP plate | InSphero, Schlieren, Switzerland | PB-CS-01-001 | |
| Ultra-low attachment (ULA) culture plates | Corning, Corning, NY, USA | 4520 | |
| airway epithelial cell growth medium | Promocell, Heidelberg, Germany | C-21060 | |
| amphotericin B | Biochrom, Berlin, Germany | A 2612 | |
| airway epithelial cell growth medium supplement mix | Promocell, Heidelberg, Germany | C39165 | |
| WST-8 test | Promocell, Heidelberg, Germany | PC PK-CA705-CK04 | |
| Keratinocyte SFMedium + L-Glutamine 500mL | Invitrogen | #17005-034 | |
| Bovine Pituitary Extract (BPE), 25mg | Invitrogen | #37000015 | |
| Recombinant human Epithelial Growth Factor 2.5 µg | Invitrogen | #37000015 | |
| DMEM High Glucose | Invitrogen | #21068-028 | |
| Penicillin Streptomycin 10000U/mL Penicillin/ 10000µg/mL Streptomycin | Invitrogen | #15140-122 | |
| F12 Nutrient Mix | Invitrogen | #21765-029 | |
| Glutamax (200 mM L-Alanyl-L-Glutamin-Dipeptide in NaCl) | Invitrogen | #35050087 | |
| HBSS (Ca, Mg) | Life Technologies | #14025-092 | (no phenol red) |
| 1x TrypLE Expres Enzyme | Invitrogen | #12604-013 | (no phenol red) |
| Accutase (enzymatic cell detachment solution) | Innovative cell technologies | Cat# AT104 | |
| 70 µm Falcon cell strainer | BD Biosciences, USA | #352350 |
Odniesienia
- Hunter, K. D., Parkinson, E. K., Harrison, P. R. Profiling early head and neck cancer. Nat Rev Cancer. 5 (2), 127-135 (2005).
- Jerjes, W., et al. The effect of tobacco and alcohol and their reduction/cessation on mortality in oral cancer patients: short communication. Head Neck Oncol. 4, 6 (2012).
- Chen, H. H. W., Kuo, M. T. Improving radiotherapy in cancer treatment: Promises and challenges. Oncotarget. 8 (37), 62742-62758 (2017).
- Boeckx, C., et al. Anti-epidermal growth factor receptor therapy in head and neck squamous cell carcinoma: focus on potential molecular mechanisms of drug resistance. Oncologist. 18 (7), 850-864 (2013).
- Brand, T. M., Iida, M., Wheeler, D. L. Molecular mechanisms of resistance to the EGFR monoclonal antibody cetuximab. Cancer Biol Ther. 11 (9), 777-792 (2011).
- Seidl, D., Schild, S. E., Wollenberg, B., Hakim, S. G., Rades, D. Prognostic Factors in Patients Irradiated for Recurrent Head-and-Neck Cancer. Anticancer Res. 36 (12), 6547-6550 (2016).
- Shirai, K., et al. Clinical Outcomes of Definitive and Postoperative Radiotherapy for Stage I-IVB Hypopharyngeal Cancer. Anticancer Res. 36 (12), 6571-6578 (2016).
- Theile, D., et al. Evaluation of drug transporters' significance for multidrug resistance in head and neck squamous cell carcinoma. Head Neck. 33 (7), 959-968 (2011).
- Slade, M. J., et al. Comparison of bone marrow, disseminated tumour cells and blood-circulating tumour cells in breast cancer patients after primary treatment. Brit J Cancer. 100 (1), 160-166 (2009).
- Mockelmann, N., Laban, S., Pantel, K., Knecht, R. Circulating tumor cells in head and neck cancer: clinical impact in diagnosis and follow-up. Eur Arch Otorhinolaryngol. 271 (1), 15-21 (2014).
- Gerlinger, M., et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 366 (10), 883-892 (2012).
- Ledgerwood, L. G., et al. The degree of intratumor mutational heterogeneity varies by primary tumor sub-site. Oncotarget. 7 (19), 27185-27198 (2016).
- Loyo, M., et al. Lessons learned from next-generation sequencing in head and neck cancer. Head Neck. 35 (3), 454-463 (2013).
- Morris, L. G., et al. The Molecular Landscape of Recurrent and Metastatic Head and Neck Cancers: Insights From a Precision Oncology Sequencing Platform. JAMA Oncol. , (2016).
- Bauml, J. M., Cohen, R. B., Aggarwal, C. Immunotherapy for head and neck cancer: latest developments and clinical potential. Ther Adv Med Oncol. 8 (3), 168-175 (2016).
- Mack, B., et al. Rapid and non-enzymatic in vitro retrieval of tumour cells from surgical specimens. PLoS One. 8 (1), e55540 (2013).
- Ham, S. L., Joshi, R., Thakuri, P. S., Tavana, H. Liquid-based three-dimensional tumor models for cancer research and drug discovery. Exp Biol Med (Maywood). 241 (9), 939-954 (2016).
- Kelm, J. M., Timmins, N. E., Brown, C. J., Fussenegger, M., Nielsen, L. K. Method for generation of homogeneous multicellular tumor spheroids applicable to a wide variety of cell types. Biotechnol Bioeng. 83 (2), 173-180 (2003).
- Kunz-Schughart, L. A., Freyer, J. P., Hofstaedter, F., Ebner, R. The use of 3-D cultures for high-throughput screening: the multicellular spheroid model. J Biomol Screen. 9 (4), 273-285 (2004).
- Lin, R. Z., Chang, H. Y. Recent advances in three-dimensional multicellular spheroid culture for biomedical research. Biotechnol J. 3 (9-10), 1172-1184 (2008).
- Weiswald, L. B., Bellet, D., Dangles-Marie, V. Spherical cancer models in tumor biology. Neoplasia. 17 (1), 1-15 (2015).
- Cancer Genome Atlas, N. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature. 517 (7536), 576-582 (2015).
- Duarte, S., et al. Isolation of head and neck squamous carcinoma cancer stem-like cells in a syngeneic mouse model and analysis of hypoxia effect. Oncol Rep. 28 (3), 1057-1062 (2012).
- Reid, P. A., Wilson, P., Li, Y., Marcu, L. G., Bezak, E. Current understanding of cancer stem cells: Review of their radiobiology and role in head and neck cancers. Head Neck. 39 (9), 1920-1932 (2017).
- Cossu, F., et al. Structural Insight into Inhibitor of Apoptosis Proteins Recognition by a Potent Divalent Smac-Mimetic. PLoS ONE. 7 (11), e49527 (2012).
- Hagemann, J., et al. Spheroid-based 3D Cell Cultures Enable Personalized Therapy Testing and Drug Discovery in Head and Neck Cancer. Anticancer Res. 37 (5), 2201-2210 (2017).
- Worp, H. B., et al. Can animal models of disease reliably inform human studies?. PLoS Med. 7 (3), e1000245 (2010).
- Wilding, J. L., Bodmer, W. F. Cancer cell lines for drug discovery and development. Cancer Res. 74 (9), 2377-2384 (2014).
- Chitcholtan, K., Asselin, E., Parent, S., Sykes, P. H., Evans, J. J. Differences in growth properties of endometrial cancer in three dimensional (3D) culture and 2D cell monolayer. Exp Cell Res. 319 (1), 75-87 (2013).
- Longati, P., et al. 3D pancreatic carcinoma spheroids induce a matrix-rich, chemoresistant phenotype offering a better model for drug testing. BMC Cancer. 13, 95 (2013).
Przedruki i uprawnienia
Zapytaj o uprawnienia na użycie tekstu lub obrazów z tego artykułu JoVE
Zapytaj o uprawnieniaPrzeglądaj więcej artyków
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. Wszelkie prawa zastrzeżone